Did you know the ACR accreditation checklist now includes a reference to AAPM Task Group 218 for patient specific QA? We spoke with Sun Nuclear medical physicist Jason Tracy, M.S., DABR, RT(T), about how sites seeking ACR accreditation or re-accreditation can prepare for the TG-218 requirement, and what this means for the field as a whole.
How did you first understand that AAPM Task Group-218 had been added as a requirement for ACR accreditation?
Over the past year, the ACR has of course been doing more audits remotely, requesting information via digital submission instead of in person, including checklists with the specific policies and procedures requested. In reviewing the checklist with a colleague, what stood out to me was a requirement for "Procedures for IMRT/VMAT patient specific QA conforming with AAPM TG-218." As far as I know, Task Group 218 had not been specifically called out by ACR in the past.
What implications does that have for sites nearing ACR accreditation?
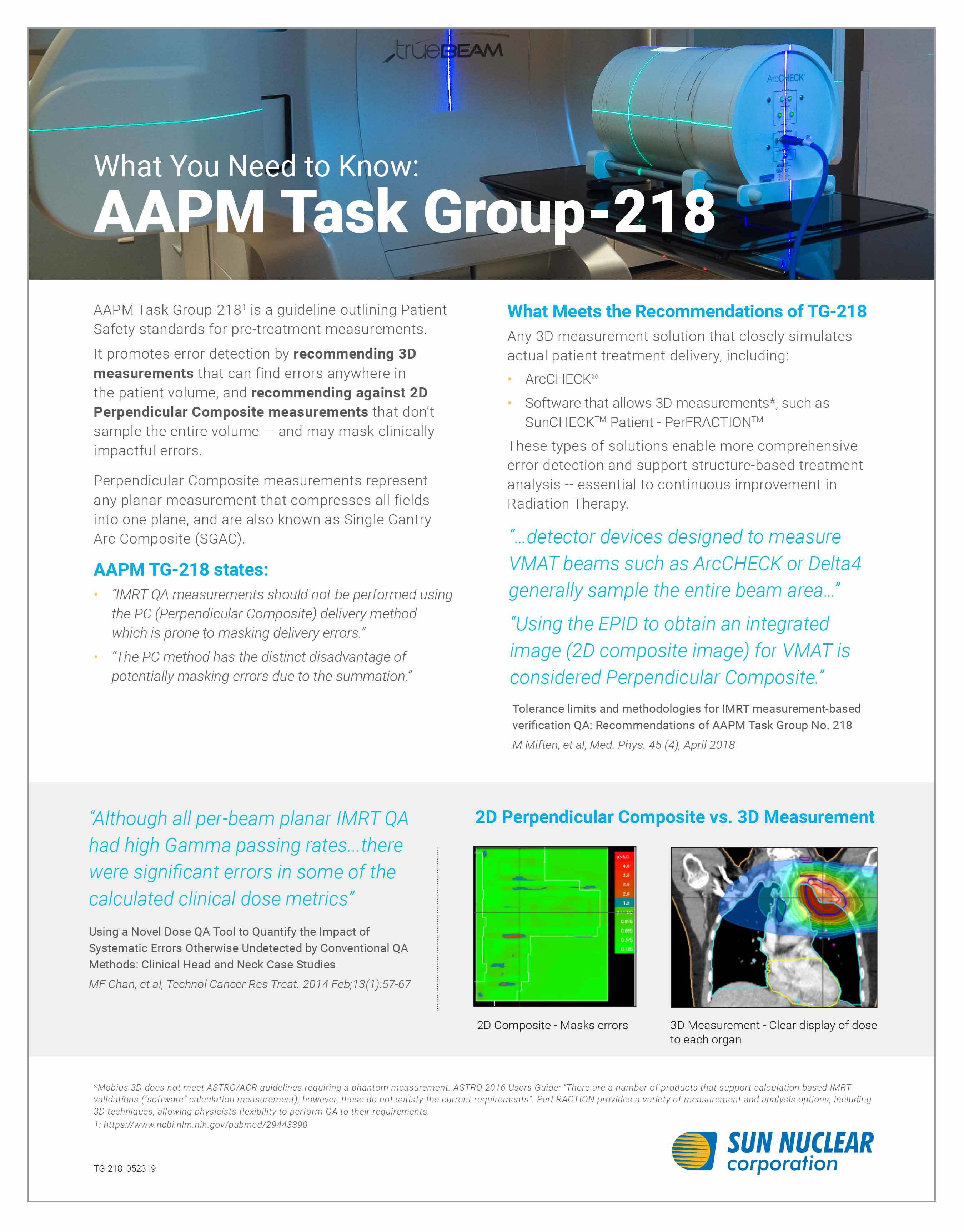
It's open to interpretation what the ACR may be looking for, but when I think of TG-218 what comes to mind are the three types of QA measurement approaches — true composite, perpendicular field-by-field, and perpendicular composite. True composite is their recommendation as the ideal way to take these measurements, followed by perpendicular field-by-field when true composite methods are not available, and they specifically state perpendicular composite techniques are not recommended as they can mask delivery errors. Another recommendation within TG-218 is utilizing criteria of 3%/2mm, so this may be something the ACR considers for this specific requirement as well.
Can you explain what they mean by true composite, perpendicular field-by-field, and perpendicular composite?
TG-218 recommends the true composite method, as this method most closely simulates the treatment delivery to the patient. 3D QA is preferred because it covers the entire field of treatment in 3D sampling throughout the field of treatment (not just in a 2D plane). Sun Nuclear's ArcCHECK array is recognized by the task group as a true composite 3D measurement device that is ideally suited for IMRT patient-specific QA, so that is one solution I recommend to sites looking to be TG-218 compliant. For a true composite 2D measurement, the task group stipulates appropriate angular corrections must be applied. Sun Nuclear's SRS MapCHECK and MapCHECK 3 arrays support this 2D true composite delivery, providing an actual dose summation in a 2D slice of the 3D dose. TG-218 discourages use of 2D arrays that do not include angular corrections for the purposes of IMRT and VMAT patient-specific QA.
In addition, the SunCHECK Dose Calculator (SDC) has been shown to have superior beam models versus similar software solutions, particularly with respect to small fields, MLC-modeling, and heterogeneity.* It also has the benefit of being fully independent. Because the software allows independent 3D measurement, SunCHECK Patient is also a good option for TG-218 compliance.
Perpendicular field-by-field delivery is another option for meeting TG-218 requirements, specifically for IMRT but not for VMAT. This involves using an array or EPID perpendicular to the beam, collecting static IMRT fields individually. While not the ideal solution per the task group, this is allowed as an IMRT pre-treatment QA approach. TG-218 considers using the EPID to obtain an integrated image for VMAT a perpendicular composite technique – even if only collecting one arc field delivery at a time. Regarding perpendicular composite, TG-218 states, “IMRT QA measurements should not be performed using the PC (perpendicular composite) delivery method which is prone to masking delivery errors.” That is to say, it is specifically not recommended to use devices and software that composite multiple beams into a 2D perpendicular plane.
What impact, if any, may this have on sites not accredited by the ACR?
Sites that are not accredited by the ACR certainly don't need to be concerned about this specific ACR requirement, but it is something for them to keep in mind. TG-218 has been around for about three years now, and the unfortunate truth is that centers not performing IMRT/VMAT patient-specific QA this way are missing errors. A composite review done in perpendicular orientation can miss errors -- this is widely understood in the field of medical physics. It's about patient safety. There's a task group supporting this thinking, and now an accreditation body as well. I anticipate this type of requirement will find its way to other accreditation bodies in the near future.
What can sites do to prepare for this requirement?
Sun Nuclear has a TG-218 infosheet that offers a quick guide to getting started. I've also included a few additional references below. Sites with specific questions can reach out to me for more information.
About Jason Tracy, MS, DABR, RT(T)
Jason Tracy is a board certified physicist who worked in the field for 10+ years before joining Sun Nuclear. He started as a therapist, went back to school for Medical Physics, and worked his way to Chief of a six-center radiotherapy group based out of Kansas. Jason streamlined QA programs across these sites and initiated two stereotactic programs. At Sun Nuclear, Jason helps clinical users of Sun Nuclear products understand how to best use these solutions in the unique setup of their sites for strong, efficient radiation therapy QA programs.
*See whitepaper "Addressing Misconceptions on IMRT Quality Assurance" for more on 3D measurement-based IMRT QA