This post was written by Christopher Bowen, MS, DABR, and originally appeared in Imaging Technology News.
The Radiation Oncology department at Missouri’s Mosaic Life Care at St. Joseph treats 50-60 patients per day and develops 25-35 treatment plans per week. Our team includes two physicians, one medical physicist, two dosimetrists and five therapists. We are a small, but very busy, team. A few years ago, we recognized an opportunity to implement stronger minimum quality standards in our clinic, specifically around SBRT and SRS treatments. In looking for tools to support this goal, our requirements were easy implementation and routine use, increased efficiency for our busy team, and positive impact to patient safety.
Today, we have a stronger stereotactic program with tools that offer more in-depth insights into our program without hindering workflow efficiency.
Stereotactic Electronic Patient QA & End-to-End Testing
To ensure a robust foundation to our stereotactic program, we use the StereoPHAN and SRS MapCHECK from Sun Nuclear. These have become invaluable tools for our center.
StereoPHAN performs testing on all aspects of stereotactic treatment, starting at CT patient setup through patient treatment. SRS MapCHECK fits into the StereoPHAN for CT simulation and stereotactic QA plan creation. The SRS MapCHECK’s angular corrections allow for highly accurate measurements to be acquired from any angle, including with Vertex fields and CyberKnife.
There have been several cases where the angular independence of the device has been helpful in catching multiple lesions on the same plane. For instance, with one particular case, the lesions from the anterior and posterior positions were not in the same plane. One lesion was oversized, while the other was not. In this case, I created a QA plan using SRS MapCHECK. With that plan stored in the system, it was obvious rotation was needed to catch both lesions optimally on the device. When adding the rotational component within the software and delivering the plan, using criteria of 2% dose difference and distance of 1 millimeter, the plan had an excellent passing rate of 97.9.
Another case that stood out was when the SRS MapCHECK detected two prominent lesions and the beginning of a third lesion. In this instance, I took a second scan with SRS MapCHECK to more accurately target the third lesion. This example really demonstrates the highly accurate measurements capable with the device, even in the gradient fall-off region. Catching a gradient dose delivery to an off-plane lesion is just as difficult, if not more so, than catching one in plane, and the SRS MapCHECK does both well.

SRS MapCHECK software image of lesions in different planes
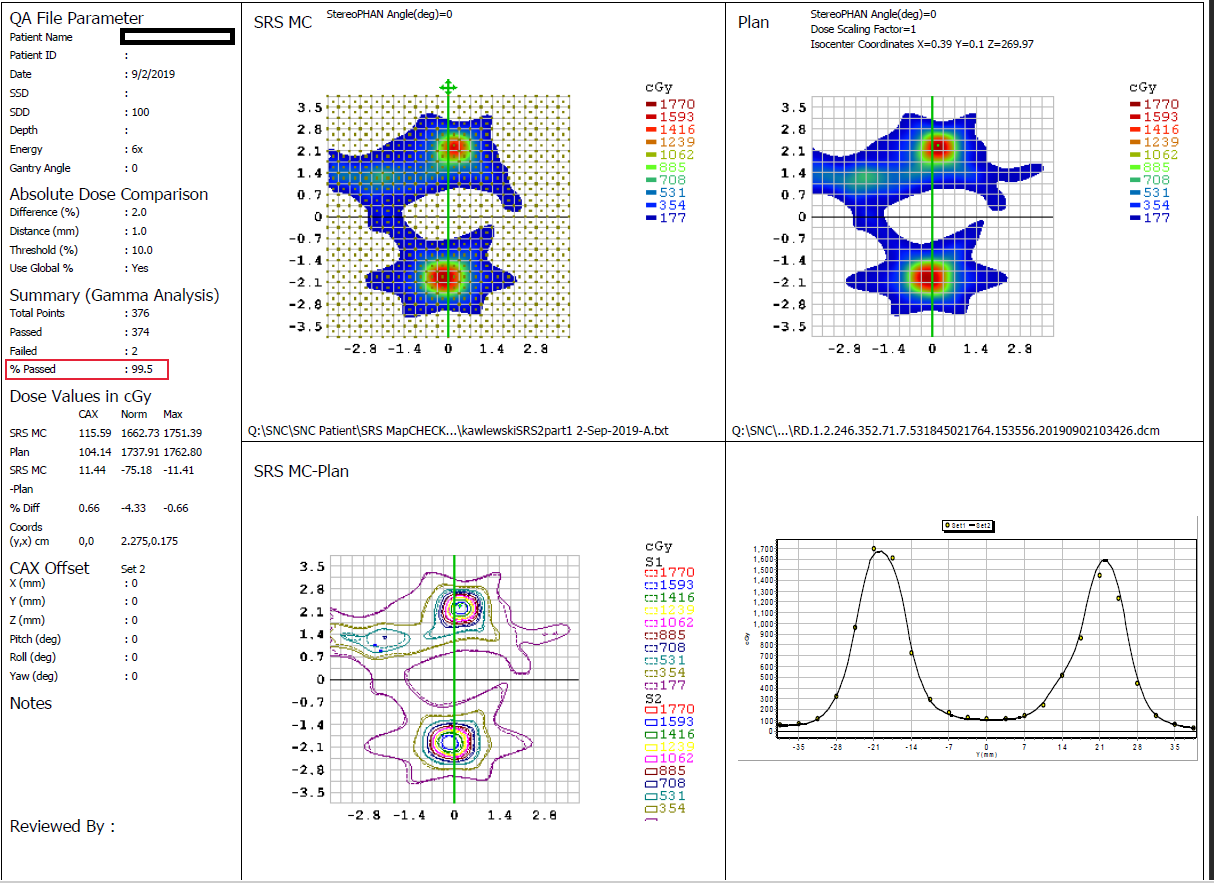
SRS MapCHECK software showing two prominent lesions and the formation of a third lesion.
Re-Thinking Isocentricity
As SBRT/SRS treatments move toward a mono-isocentric approach, programs can no longer solely rely on their machine’s performance at a single point. Typically, when commissioning and accepting linacs that will deliver high-dose plans, we are demonstrating isocentricity at isocenter. This presents a unique challenge for the field, because some mono-isocentric treatments may be beyond two or three centimeters from isocenter.
When your machine is only guaranteed to perform at isocenter and the vendor doesn’t provide a specification or test for off-axis accuracy, how can you determine and monitor the accuracy for off-axis tumors? This becomes a major issue with single isocenter multi-met plans.
Enter the MultiMet-WL Cube phantom.
The MultiMet-WL Cube is similar to Sun Nuclear’s standard Winston-Lutz cube, but elongated and with several BB’s offset at specific distances.
Initial Experience
As an early user of this tool, I first completed a standard Winston-Lutz test, followed by a test using the MultiMet-WL Cube. It was eye-opening to see all the errors found with the new cube that were not found with the standard Winston-Lutz cube. With this new information, I re-ran the TrueBeam IsoCal test, reapplying the cone beam and retreating the plan to the phantom. After doing so, the detected errors were significantly reduced.
These findings made our QA team question how often we should perform IsoCal tests and isocenter verification. For departments performing single isocenter multi-met treatments, this is an important dialogue for your team.
Ultimately, we found that we had better insight into the performance of our machine’s limitations. Even if a machine has limitations past the three- or four-centimeter range, that does not necessarily mean that department cannot perform multi-met isocenter treatments. In these instances, it is advisable to add an extra isocenter. It’s my opinion that the time required to add another isocenter is a fair trade-off for having confidence the machine is performing within expected tolerances for lesions further away from isocenter.
Bringing Together the SRS Program
Together, the StereoPHAN, SRS MapCHECK, and MultiMet-WL Cube provide an invaluable bird’s eye view of a linear accelerator’s capabilities for stereotactic treatments. The dose overlays in the software are strict enough that it’s obvious when plans require adjustments. I rely on these tools for all my stereotactic cases. I have full confidence with the SRS MapCHECK as a surrogate for a patient, and the MultiMet-WL Cube provides additional safeguards for off-axis lesions.
Getting Setup
These tools are simple to setup and use. For SRS MapCHECK, complete array calibration, scanning, and software setup took just one afternoon. For the MultiMet-WL Cube, setup entails using provided treatment plans, and then loading and delivering the plan. This process takes approximately 10-15 minutes in total, and software produces off-axis accuracy results within a minute.
Before delivery, I recommend positioning them with a cone-beam (or however you setup your patients) to keep the test mimicking patient treatment. Once you’ve delivered the results, open the MultiMet-WL Cube software and click on any one file; the software will automatically process the images.
Accelerate Workflows
For stereotactic and conventional deliveries, as a small department treating many patients daily, keeping organized and working efficiently are extremely important. For this reason, we use SunCHECK as a single source of management of our QA data.
The Machine QA portion of SunCHECK nicely organizes daily, monthly and annual QA, with the ability to easily investigate tests that are failing. Within five minutes of logging on in the morning, I can see from the SunCHECK dashboard how all my equipment is performing.
Likewise, the dashboard also shows Patient QA results at-a-glance, including initial dose check, 3-D analysis with DVH, pre-treatment EPID QA, and in-vivo monitoring. It is the most practical, complete 3-D solution available for measured QA of multi-met cases.
Having insights into how successful treatment is on the first fraction and in subsequent fractions provides information we didn’t have previously. As the field advances toward adaptive care, SunCHECK offers measurable evidence Medical Physicists can use to influence decision-making during the treatment plan.
About the Author
Christopher Bowen, M.S., DABR, is a Board-Certified Medical Physicist at Mosaic Life Care at St. Joseph. He has extensive experience with cranial SRS treatments using the Varian Medical Systems® HyperArc™ System.